

The federal government classifies communities with fewer than one primary care provider for every 3,500 residents as health professional shortage areas. Of Texas’ 254 counties, just 30—most of which are in metropolitan areas—do not have provider shortages, according to the Rural Health Information Hub.
The overview
Texas nurse practitioners must sign an annual contract and pay a fee to a supervising physician, who oversees patient care through in-person or virtual meetings at least once a month. Ten other states have similar laws, according to the American Association of Nurse Practitioners.Erin Pérez, president of the professional organization Texas Nurse Practitioners, said some nurse practitioners who graduate from Texas universities choose to work in telemedicine or move to other states to avoid the “regulatory burden,” contributing to the health care workforce shortage. Over 72% of nurse practitioners in Texas are licensed in primary care, according to a 2022 report from TNP.
“[This regulation] takes from patients' finances because somebody's having to pay for it. So even if they're in the hospital, or they're in a nursing home, or they're in a rehab, ... somebody is paying that physician signature fee that does not improve their care and doesn't improve their quality outcomes,” Pérez said.
The details
Nurse practitioners must receive a master's or doctoral degree, undergo clinical training and get a national board certification before they can begin caring for patients. However, they do not have to complete a multiyear residency program, which is required for physicians.
TNP has advocated for independent practice legislation for several legislative sessions, with bipartisan support from lawmakers. On the other side, the Texas Medical Association has defended the current regulations, arguing physician-led teams are essential to protect patients.
“I never want to stop a nurse practitioner from graduating and performing at the highest level of their license,” TMA President Dr. Ray Callas said. “The solution [to the provider shortage] is not allowing a nurse practitioner to have independent practice. What that is doing is, now you're lowering the standard of care that we provide for every Texan.”
Nurse practitioners argue the current supervision requirements do not benefit patients. The law states a nurse practitioner and supervising physician must have check-in meetings at least once a month to discuss patient care.
“You don't have to be at the same practice site; you don't have to be at the same office; you don't even have to be in the same county,” said Erin Cusack, the director of government affairs for TNP. “You don't have to be in the same specialty; they don't have to see or provide care to your patients. None of those things are required at all—it's just that monthly call and that retrospective chart review.”
Callas said he would like to see physicians providing more oversight and collaborating more with the nurse practitioners they supervise.
Zooming in
Pérez has three national board certifications and works in palliative care for University Health in San Antonio. Pérez’s employer pays her supervising physicians.
She said she would like to open her own clinic but cannot afford to pay a potentially large fee while supporting her family. There are no limits on how much physicians can charge, Pérez said.
“What other profession has a signature fee as large as six figures, only a signature, and it doesn't improve productivity? ... This pay-to-play model is just, it's not right, and it's not helpful. It's detrimental to our patients; it's detrimental to our health care systems,” Pérez said.
If a supervising physician retires or dies, nurse practitioners must stop treating patients until they can sign a new contract.
“We’re talking like two-to-three thousand patients [who], in one instant, don't have access to their nurse practitioner because that delegating physician retired or died—it’s incredible,” Pérez said. “That's the heart stop of any nurse practitioner business owner: ‘What happens if that physician that I'm delegating with and paying all of a sudden is no more? What then? How do I help my patients that I've been caring for get that access to care, get their medications that keep them as healthy as we can?’”
Callas said the Texas Medical Association’s primary concern is the gap in training between physicians and nurse practitioners.
“There’s nothing comparable between a physician and a nurse practitioner based on education, also based on experience. ... I'm talking tens to hundreds of thousands of hours [of training] that we receive, is not the same as a nurse practitioner that just basically does their class online,” Callas said. “We don't think that nurse practitioners should not be a part of the health care team, but practicing independently without the proper expertise and training is something that we definitely do not believe in.”
Cusack said allowing nurse practitioners to work independently would not take business from physicians but would help more Texans access health care.
“There is no world in which you do not need physicians,” Cusack said. “[Nurse practitioners] are like the front door of the health care system, and physicians are needed for all of the complicated cases that come along the way—for procedures, for surgery, for specialty—and they work in collaboration and teamwork together, so it's not a threat.”
By the numbers
Last year, Texas ranked 51st in the nation for access to and affordability of health care, according to the Commonwealth Fund, a health care foundation.
The number of Texans applying for a medical license has steadily increased each year, but the state still has “a serious shortage of physicians,” according to the TMA. Texas has 8.8% of the U.S. population and 7.3% of active U.S. physicians, the medical association reported in 2022.
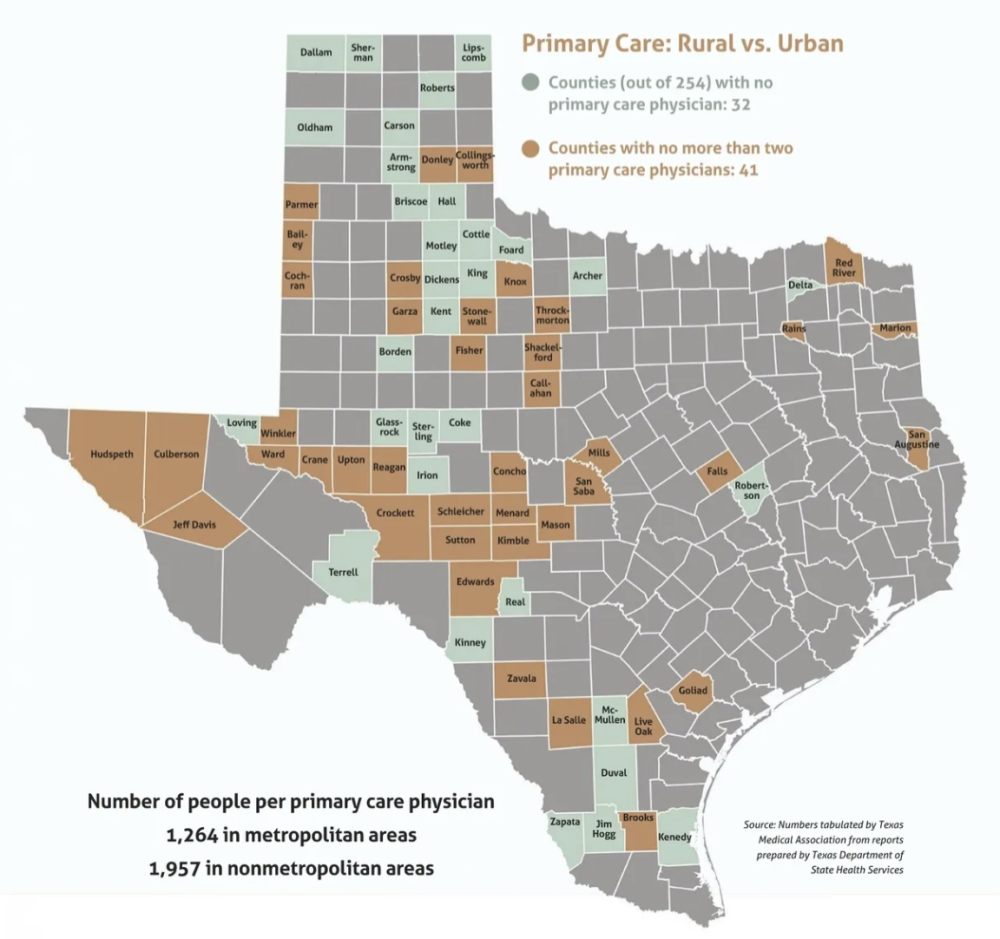
Shortages are particularly dire in rural areas, where hospitals sometimes close due to a lack of employees. Of Texas’ 254 counties, 32 had no primary care physicians in 2022, and 41 had no more than two primary care physicians, according to the TMA report.
“We want to make sure that we have internet ... throughout the state of Texas,” Callas said. “That would help tremendously—if people have broadband access to the internet, we might be able to make access easier from the telemedicine standpoint.”
Researchers from Texas A&M University found allowing nurse practitioners to work independently would generate over 4,000 new jobs in Texas and reduce the primary care provider shortage by 32%.
The study showed that in 2022, there were 124 Texas counties with more primary care nurse practitioners than physicians, 81 of which were rural. There were more physicians than nurse practitioners in 91 counties, 58 of which were rural; and 22 counties had roughly equal quantities of each provider.
Eliminating supervisory requirements “is a no-cost way to significantly expand access to care,” according to the study, because patients are typically charged less for care from a nurse practitioner than a physician.
“My hope is in my lifetime that Texans will get that basic human right of primary and mental health care, women's health care,” Pérez said. “You know, I'm not asking to do brain surgery—I'm just asking to do what I'm educated and trained, licensed and certified to do.”
Stay tuned
Ahead of the 2025 legislative session, which begins in January, Lt. Gov. Dan Patrick asked state senators to look into “whether regulatory and licensing flexibilities could improve access to care, particularly in medically underserved areas of Texas ... while maintaining patient safety.”
The Senate Health and Human Services Committee is scheduled to discuss this topic during a Sept. 18 meeting. The committee will not vote or take immediate action on any agenda items but can make recommendations for next year’s legislation.